
summary
The European Resuscitation Council (ERC) and the European Society of Critical Care Medicine (ESICM) have collaborated to develop these post-resuscitation care guidelines for adults, in line with the 2020 International Consensus on the Science and Treatment of CPR. Topics covered include post-cardiac arrest syndrome, diagnosis of causes of cardiac arrest, oxygen and ventilation control, coronary infusion, hemodynamic monitoring and management, seizure control, temperature control, general intensive care management, prognosis, long-term outcomes, rehabilitation, and organ donation.
Keywords: Cardiac arrest, postoperative resuscitation care, prediction, guidelines
Introduction and scope
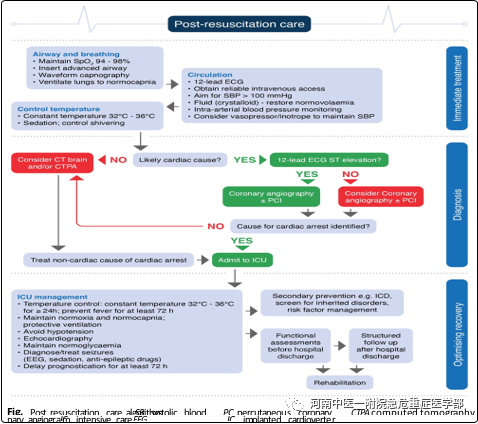
In 2015, the European Resuscitation Council (ERC) and the European Society of Critical Care Medicine (ESICM) collaborated to develop the first joint post-resuscitation care guidelines, which were published in Resuscitation and Critical Care Medicine. These post-resuscitation care guidelines were extensively updated in 2020 and incorporate science published since 2015. Topics covered include post-cardiac arrest syndrome, oxygen and ventilation control, hemodynamic targets, coronary infusion, targeted temperature management, seizure control, prognosis, rehabilitation, and long-term outcomes (Figure 1).
Summary of major changes
Immediate post-resuscitation care:
• Post-resuscitation treatment begins immediately after sustained ROSC (recovery of spontaneous circulation), regardless of location (Figure 1).
• For out-of-hospital cardiac arrest, consider taking a cardiac arrest center. Diagnose the cause of cardiac arrest.
• If there is clinical (e.g., hemodynamic instability) or ECG evidence of myocardial ischemia, coronary angiography is performed first. If coronary angiography does not identify the causative lesion, CT encepography and/or CT pulmonary angiography are performed.
• Early identification of respiratory or neurological disorders can be done by performing CT scans of the brain and chest during hospitalization, before or after coronary angiography (see Coronary Reperfusion).
• Perform CT of the brain and/or angiography of the lungs if there are signs or symptoms suggestive of a neurological or respiratory cause prior to asystole (e.g., headache, epilepsy, or neurological deficits, shortness of breath, or hypoxemia documented in patients with known respiratory conditions).
1. Airway and breathing
Airway management after spontaneous circulation has been restored
• Airway and ventilatory support should be continued after recovery of spontaneous circulation (ROSC).
• Patients who have had transient cardiac arrest, immediate return to normal brain function, and normal breathing may not require endotracheal intubation, but should be given oxygen through a mask if their arterial oxygen saturation is less than 94%.
• Endotracheal intubation should be performed in patients who remain comatose after ROSC, or for patients with other clinical indications for sedation and mechanical ventilation, if endotracheal intubation is not performed during CPR.
• Endotracheal intubation should be performed by an experienced operator with a high success rate.
• Correct placement of the endotracheal tube must be confirmed by a waveform capnography.
• In the absence of experienced endotracheal intubators, it is reasonable to insert a supraglottic airway (SGA) or maintain the airway using basic techniques until a skilled intubator is available.
Oxygen control
• After ROSC, 100% (or maximally available) oxygen is used until arterial oxygen saturation or arterial partial pressure of oxygen can be reliably measured.
• Once the arterial oxygen saturation can be reliably measured or the arterial blood gas value can be obtained, the inspired oxygen is titrated to achieve an arterial oxygen saturation of 94-98% or an arterial partial pressure of oxygen (PaO2) of 10 to 13 kPa or 75 to 100 mmHg (Figure 2).
• 避免ROSC后的低氧血症(PaO2 < 8 kPa或60 mmHg)。
• Avoid hyperxemia after ROSC.

Ventilation control
• Obtain arterial blood gases and use end-tidal CO2 monitoring in mechanically ventilated patients.
• For patients requiring mechanical ventilation after ROSC, adjust ventilation to achieve a normal arterial partial pressure of carbon dioxide (PaCO2) of 4.5 to 6.0 kPa or 35 to 45 mmHg.
• PaCO2 is frequently monitored in patients treated with targeted temperature management (TTM) because hypocapnia may occur.
• Blood gas values are always measured using temperature or non-temperature correction methods during TTM and low temperatures.
• Adopt a lung-protective ventilation strategy to achieve a tidal volume of 6 – 8 ml/kg of ideal body weight.
2. Coronary circulation
Reperfusion
• Adult patients with ROSC following suspicion of cardiac arrest and ST-segment elevation on ECG should undergo urgent cardiac catheterization laboratory evaluation (PCI should be performed immediately if indicated).
• Urgent cardiac catheterization laboratory evaluation should be considered in patients with ROSC who have an out-of-hospital cardiac arrest (OHCA) without ST-segment elevation on ECG and who are estimated to have a high probability of acute coronary artery occlusion (e.g., haemodynamic and/or electrically unstable patients).
Haemodynamic monitoring and management
• Continuous monitoring of blood pressure through the ductus arteriosus should be performed in all patients, and cardiac output monitoring is reasonable in haemodynamically unstable patients.
• Perform an echocardiogram as early (as soon as possible) in all patients to identify any underlying cardiac conditions and to quantify the degree of myocardial dysfunction.
• Avoid hypotension (< 65 mmHg). Target mean arterial pressure (MAP) to achieve adequate urine output (> 0.5 mL/kg*h and normal or reduced lactate (Figure 2).
• Bradycardia can be left untreated during TTM at 33°C if blood pressure, lactate, ScvO2, or SvO2 are sufficient. If not, consider increasing the target temperature, but not higher than 36°C.
• Maintenance perfusion with fluids, norepinephrine, and/or dobutamine depending on the need for intravascular volume, vasoconstriction, or muscle contraction in the individual patient.
• Avoid hypokalemia, which is associated with ventricular arrhythmias.
• If fluid resuscitation, muscle contraction, and vasoactive therapy are inadequate, mechanical circulatory support (eg, intra-aortic balloon pump, left ventricular assist device, or arteriovenous extracorporeal membrane oxygenation) may be considered for the treatment of persistent cardiogenic shock due to left ventricular failure. Left ventricular assist devices or extracorporeal endovascular oxygenation should also be considered in patients with haemodynamically unstable acute coronary syndrome (ACS) and recurrent ventricular tachycardia (VT) or ventricular fibrillation (VF), despite optimal treatment options.
3. Motor function (optimize neurological recovery)
Control seizures
• We recommend the use of electroencephalogram (EEG) to diagnose electrospasms in patients with clinical convulsions and to monitor the response to treatment.
• To treat seizures after cardiac arrest, we suggest levetiracetam or sodium valproate as first-line antiepileptic drugs in addition to sedative medications.
• We recommend not using routine seizure prophylaxis in patients following cardiac arrest.
Temperature control
• For adults who do not respond to OHCA or in-hospital cardiac arrest (any initial heart rhythm), we suggest targeted temperature management (TTM).
• Keep the target temperature at a constant value between 32 and 36 °C for at least 24 hours.
• For patients who remain comatose, avoid fever (> 37.7°C) for at least 72 hours after ROSC.
• Do not use prehospital intravenous cold solution to lower body temperature. General Intensive Care Management – Use of short-acting sedatives and opioids.
• Routine use of neuromuscular blocking drugs is avoided in patients with TTM, but may be considered in cases of severe chills during TTM.
• Stress ulcer prophylaxis is routinely provided to patients with cardiac arrest.
• Prevention of deep vein thrombosis.
• 如果需要,使用胰岛素输注将血糖定位为7.8-10 mmol/L(140- 180 mg/dL),避免低血糖(<4.0 mmol/L(< 70 mg/dL)。
• Start low-rate enteral feeds (nutritional feeding) during TTM and increase after rewarming if needed. If a TTM of 36°C is used as the target temperature, the enteral feeding rate may increase earlier during the TTM.
• We do not recommend routine use of prophylactic antibiotics.

4. Conventional forecasting
General guidelines
• We do not recommend prophylactic antibiotics for patients who are unconscious after resuscitation from cardiac arrest, and neuroprognosis should be performed by clinical examination, electrophysiology, biomarkers, and imaging, both to inform the patient’s relatives and to help clinicians target treatment based on the patient’s chances of achieving meaningful neurological recovery (Figure 3).
• No single predictor is 100% accurate. Therefore, we recommend a multimodal neural prediction strategy.
• When predicting poor neurological outcomes, high specificity and accuracy are required to avoid false pessimistic predictions.
• Clinical neurological examination is essential for prognosis. To avoid erroneously pessimistic predictions, clinicians should avoid potential confounding of test results that can be confound by sedatives and other medications.
• Daily clinical examination is advocated when patients are treated with TTM, but the final prognostic assessment should be performed after rewarming.
• Clinicians must be aware of the risk of self-induced prophecy bias, which occurs when index test results predicting poor outcomes are used in treatment decisions, particularly with regard to life-sustaining therapies.
• The purpose of the Neuroprognosis Index test is to assess the severity of hypoxic-ischemic brain injury. Neuroprognosis is one of several aspects to consider when discussing an individual’s potential for recovery.
Multi-model forecasting
• Begin prognostic assessment with an accurate clinical examination, performed only after major confounding factors (e.g., residual sedation, hypothermia) have been excluded (Figure 4)
• In the absence of confounders, comatose patients with ROSC ≥ M≤3 within 72 hours are likely to have poor outcomes if two or more of the following predictors are present: no pupillary corneal reflex at ≥ 72 h, bilateral absence of N20 SSEP ≥ 24 h, high-grade EEG > 24 h, specific neuronal enolase (NSE) > 60 μg/L for 48 h and/or 72 h, state myoclonus ≤ 72 h, or diffuse brain CT, MRI and extensive hypoxic injury. Most of these signs can be recorded before 72 h of ROSC; However, their results will only be assessed at the time of clinical prognostic assessment.

Clinical examination
• Clinical examination is susceptible to interference from sedatives, opioids, or muscle relaxants. Possible confounding by residual sedation should always be considered and ruled out.
• For patients who remain in a coma 72 hours or later after ROSC, the following tests may predict a worse neurological prognosis.
• In patients who remain comatose 72 hours or later after ROSC, the following tests may predict adverse neurological outcomes:
– Absence of bilateral standard pupillary light reflexes
– Quantitative pupilometry
– Loss of corneal reflex on both sides
– Myoclonus within 96 hours, especially state myoclonus within 72 hours
We also recommend recording an EEG in the presence of myoclonic tics in order to detect any associated epileptiform activity or to identify EEG signs, such as background response or continuity, suggesting potential for neurological recovery.

neurophysiology
• EEG (electroencephalogram) is performed in patients who lose consciousness after cardiac arrest.
• Highly malignant EEG patterns include suppression backgrounds with or without periodic discharges and burst suppression. We recommend using these EEG patterns as an indicator of poor prognosis after the end of TTM and after sedation.
• The presence of definite seizures on EEG in the first 72 hours after ROSC is an indicator of poor prognosis.
• Lack of background response on EEG is an indicator of poor prognosis after cardiac arrest.
• Bilateral somatosensory-induced loss of cortical N20 potential is an indicator of poor prognosis after cardiac arrest.
• The results of EEG and somatosensory evoked potentials (SSEP) are often considered in the context of clinical examination and other examinations. Neuromuscular blocking drugs must be considered when SSEP is performed.
Biomarkers
• Use a range of NSE measurements in combination with other methods to predict outcomes after cardiac arrest. Elevated values at 24 to 48 hours or 72 hours, combined with high values at 48 to 72 hours, indicate a poor prognosis.
Imaging
• Use brain imaging studies to predict poor neurological outcomes after cardiac arrest in combination with other predictors in centers with relevant research experience.
• The presence of generalized cerebral edema, manifested by a marked reduction in the gray/white matter ratio on brain CT, or widespread diffusion limitation on brain MRI, predicts poor neurological prognosis after cardiac arrest.
• Imaging findings are often considered in combination with other methods to predict neurological prognosis.
5. Stop life-sustaining treatment
• Separate discussion of the prognosis assessment of withdrawal and neurological recovery of life-sustaining therapy (WLST); The decision to WLST should take into account aspects other than brain injury, such as age, comorbidity, systemic organ function, and patient selection.
Allocate adequate time for communication, long-term prognosis after cardiac arrest
The level of treatment within the team determines and • conducts physical and non-relative functional assessments with relatives. Early detection of rehabilitation needs for physical impairments prior to discharge and provision of rehabilitation services when needed. (Figure 5).

• Organize follow-up visits for all cardiac arrest survivors within 3 months of discharge, including the following:
- 1. Screen for cognitive problems.
2. Screen for mood problems and fatigue.
3. Provide information and support to survivors and families.
6. Organ donation
• All decisions regarding organ donation must comply with local legal and ethical requirements.
• Organ donation should be considered for those who meet ROSC and meet criteria for neurological death (Figure 6).
• In comatologically ventilated patients who do not meet criteria for neurological death, organ donation should be considered at the time of circulatory arrest if the decision is made to start end-of-life treatment and discontinue life support.
Post time: Jul-26-2024